We talk about a stroke when certain parts of the brain had a lack of oxygen, resulting in impaired neurological function. The symptoms depend on the affected part of the brain. There might be a paresis, a loss of sensation or vision, difficulty with speech, dizziness, …. In case of a TIA (transient ischaemic attack) the symptoms last less than 24 hours, because the oxygen supply restores spontaneously.
A stroke might be caused by a bleeding in brain tissue (haemorrhagic stroke) or by a blood clot obstructing a blood vessel (ischaemic stroke). Most of the strokes are ischaemic. Usually on admission a CT scan is done to exclude a haemorrhage and to search for major blood clots. If an ischaemic stroke is suspected and the patient is in the hospital less than 4.5 hours after onset, medication can be administered trying to resolve the blood clot (thrombolysis). If this medication fails and if a blood clot is clearly visible on imaging, the clot can be removed mechanically (thrombectomy).
In case of a (suspected) stroke or TIA, people should be admitted to the stroke unit and have a broad cardiovascular check-up. Usually a MRI scan is done to get more detailed imaging of the brain and to specify the affected brain region(s).
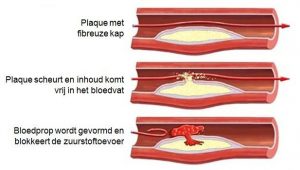
Most of the strokes or TIA’s are caused by a clot obstructing a blood vessel. As part of the check-up we test blood samples. In young patients a clotting disorder might be the cause of the stroke. In many older patients, a clot is formed by atherosclerosis. This is a slowly occurring process of growing fat (mainly cholesterol) deposits in arterial vessel walls, forming a ‘plaque’. The plaque might grow and obstruct the blood vessel or more frequently disrupt, making a blood clot obstructing the vessel. Sometimes a small particle of a blood clot gets loose (embole) and obstructs another blood vessel downstream.
Because atherosclerosis is promoted by high blood pressure, diabetes, smoking and high levels of cholesterol in the blood, these factors are all checked during admission.

Usually the cervical blood vessels (the ones in the neck), are imaged. In case of a major narrowing, surgery might be necessary to restore blood flow.
The heart is checked by echography and the heart rhythm is registered by monitor and a 24 hour registration (holter). Some arrhythmias (commonly atrial fibrillation) increase the risk of forming small blood clots in the heart (emboles).
The above mentioned examinations, help us to prevent the occurrence of a new stroke or TIA. Usually medication is started to prevent blood clotting eg aspirine, clopidogrel or direct anticoagulants. To rehabilitate, physiotherapy, ergotherapy and/or speech therapy are started. If necessary, the patient should be transferred from the stroke unit to a rehabilitation centre.
Dr Hauth has a special interest in stroke.